A previously healthy 67-year-old man presented to an otolaryngology department with progressively worsening sore throat over several weeks, unintentional 5-kg weight loss, and night sweats, according to a case report
In the report, published online in JAMA Otolaryngology–Head & Neck Surgery, researchers noted that initial physical examination revealed a mobile, nontender left-sided jugular lymph node, while dentition and oropharyngeal examinations were unremarkable. Flexible laryngoscopy showed normal results. Laboratory findings indicated elevated C-reactive protein and polyclonal elevation of gamma globulins, with normal complete blood cell count, kidney markers, and liver enzymes.
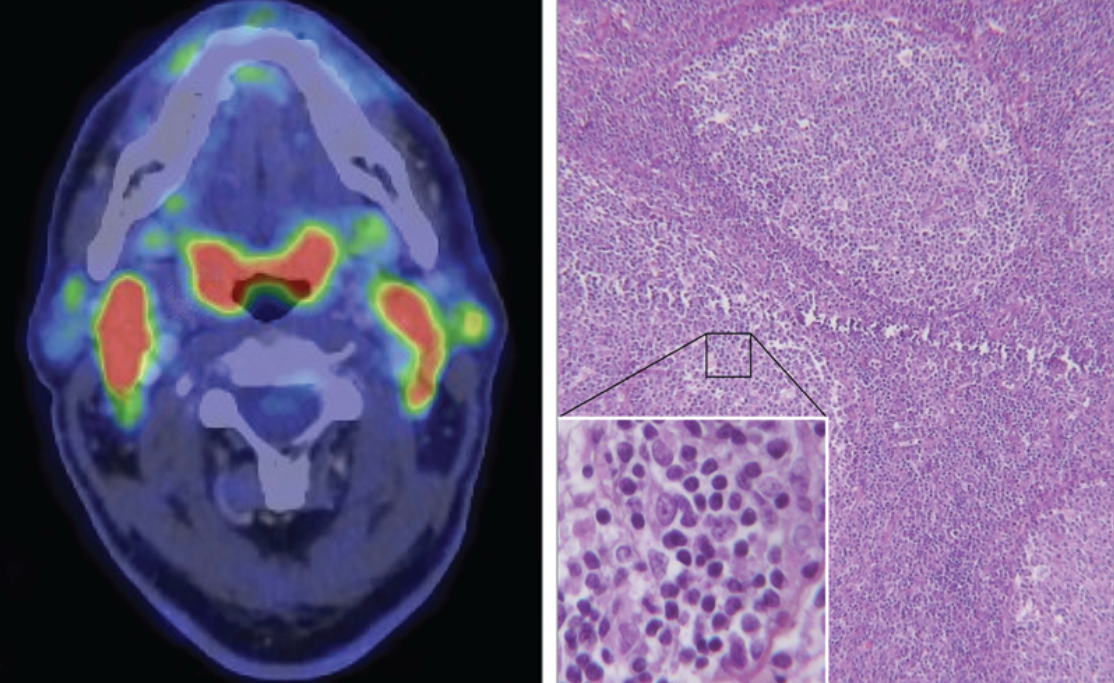
When the patient's symptoms substantially worsened over subsequent weeks, positron emission tomography/computed tomography (PET/CT) was performed, revealing "intense bilateral tonsillar hypermetabolism and abnormal lymph node hypermetabolism above and below the diaphragm," the study authors reported.
Diagnostic Challenge
The patient underwent unilateral tonsillectomy followed by antibiotics and prednisone. Pathologic examination initially showed "lymphoid follicular hyperplasia associated with a polymorphic inflammatory infiltrate without abnormal lymphoid cells and plasmocytes."
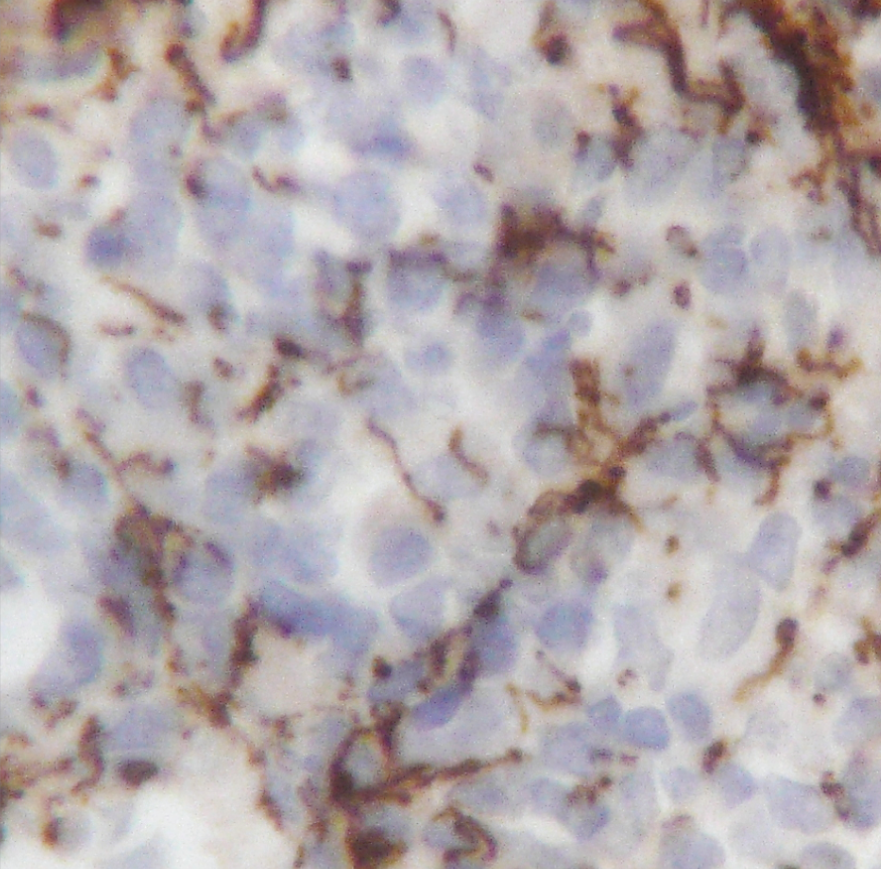
It wasn't until nearly a year after initial presentation that a pathology review of the tonsils discovered strong positive immunostaining of antitreponemal antibody associated with a rapid plasma reagin (RPR) blood titer of 1:4. A treponemal antibody test (chemiluminescent immunoassay) confirmed the diagnosis of syphilis.
Treatment and Resolution
Following diagnosis, the patient "received intramuscular injections of 2.4 million units of benzathine penicillin G once [per] week for 3 weeks, with rapid and complete regression of his symptoms."
Clinical Significance
The case report highlighted the increasing incidence of syphilis in high-income countries and its varied presentations. The researchers indicated that "syphilis of the tonsils rarely presents as a symptom of secondary syphilis. At this stage, the condition presents as bilateral tonsillitis rather than unilateral tonsillitis, as in primary syphilis."
The researchers emphasized that "although tonsils usually exhibit redness, swelling, and a gray exudate, often with a diffuse pharyngitis, initial clinical examination can be normal, and tonsillitis is only revealed by [PET]/CT."
Diagnostic Considerations
The researchers cautioned that confirmation with treponemal antibody testing is required "because of [the] high false positivity rate of RPR, up to 15%, and treponemal immunohistochemical stain is not specific of Treponema pallidum and can cross-react with commensal spirochetes of the gastrointestinal tract."
A detailed sexual history might also guide laboratory workup, as "syphilis cases are increased among men who have sex with men," though the patient reported only heterosexual intercourse.
The case reinforced why syphilis is often called "the great masquerader," according to the study authors. They concluded that "given this and the increasing incidence of syphilis, a nontreponemal blood test could be included in the diagnostic approach when facing persistent sore throat and lymphadenopathy."
The authors declared having no competing interests.