A 12-year-old boy with a 5-year history of a nonprogressive hyperpigmented plaque on his right forearm was diagnosed with pigmented dermatofibrosarcoma protuberans (Bednar tumor), a rare variant that accounts for just 1% to 5% of all dermatofibrosarcoma protuberans cases.
The patient, whose case was reported by Ruba Srour, MD, and colleagues at Rambam Health Care Campus, presented with a hyperpigmented and indurated plaque on his right forearm without any other medical conditions. Histopathological evaluation revealed monomorphic spindle cells throughout the dermis that extended into subcutaneous fat in storiform and honeycomb patterns. Pigmented cells presented in one of the fascicles.
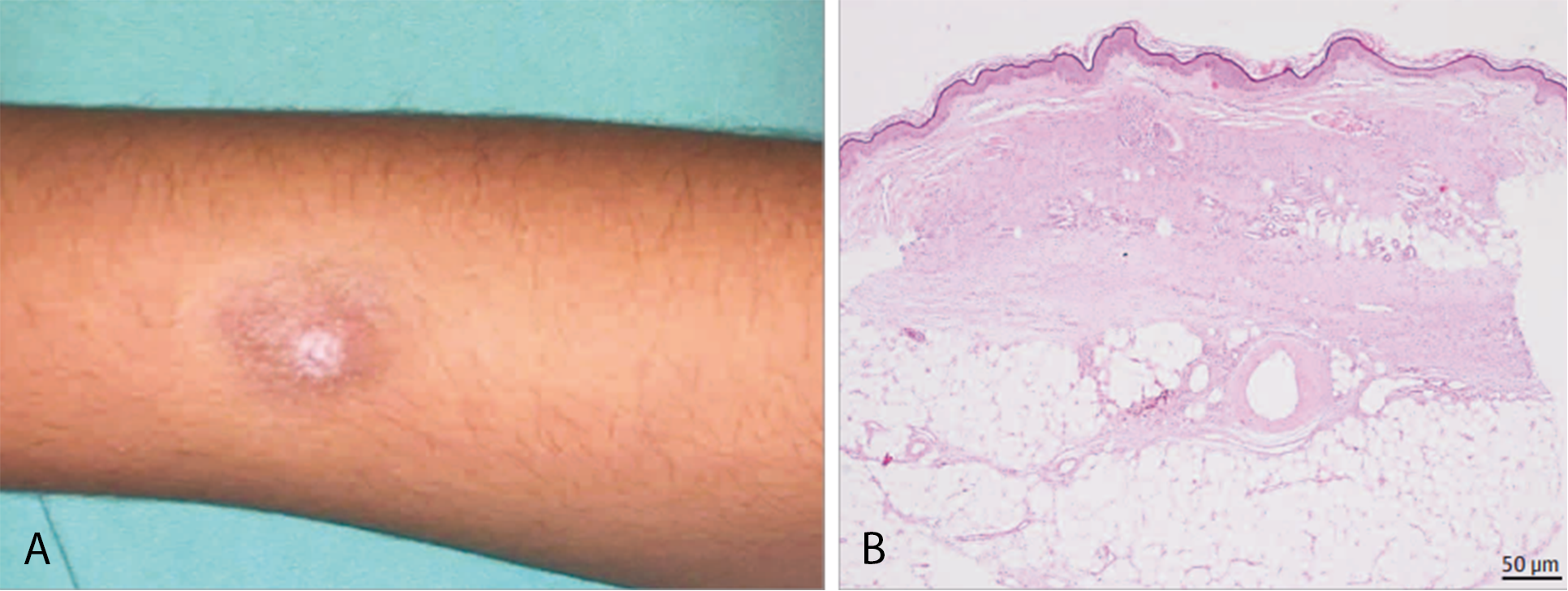
Immunohistochemical staining was positive for CD34 in spindle cells, while Melan-A, HMB45, and S100 stained only the pigmented cells. Molecular testing confirmed the presence of t(17;22)(q22;q13) translocation, resulting in a fusion gene between COL1A1 and PDGFB.
What's Your Diagnosis?
A. Dermatofibroma
B. Pigmented dermatofibrosarcoma protuberans (DFSP; Bednar tumor)
C. Desmoplastic melanoma
D. Morphea
Diagnosis and Clinical Course
Bednar tumor is a distinctive pigmented variant of DFSP that is characterized by monomorphic spindle-shaped cells intermingled with melanin-containing cells. The tumor typically presents as a slow-growing bulging lesion, primarily on the extremities. Metastasis is rare and late, and occurs via hematogenous routes, mainly to the lungs.
The origin of the tumor cells remains undetermined, though they may be derived from neuroectodermal cells based on ultrastructural and immunohistochemical findings and the presence of melanosome-containing cells.
On the molecular level, Bednar tumors are characterized by t(17;22)(q22;q13) translocation, leading to fusion between the genes COL1A1 and PDGFB. The fused gene results in overexpression of PDGFB, leading to cellular proliferation and tumor formation.
The patient underwent complete surgical excision followed by Mohs micrographic surgery and maintained complete remission after 3 years of follow-up. Ensuring negative margins in Mohs micrographic surgery is considered the standard of care for DFSP treatment because inadequate resections may result in high rates of local recurrence.
Differential Diagnosis
Dermatofibroma of the hemosiderotic variant may appear as a hardened pigmented plaque, simulating pigmented DFSP. Pathologically, it shows spindle and fusiform fibro-histiocytic cells with scattered hemosiderin-laden multinucleated giant cells. The cells stain positively for factor XIII, A chain, but negatively for CD34.
Desmoplastic melanoma is a rare variant of malignant melanoma that appears as a slowly enlarging area of thickened skin, sometimes described as a scarlike neoplasm, which may be pigmented. Histologically, pauci-cellular atypical spindle cells separated by fibro-collagenous stroma are typical. S100 and Sox10 stains are usually positive, whereas HMB45 and Melan-A stains are mostly negative.
Burnt out morphea may appear as a pigmented plaque but is not characterized by CD34+ spindle cell proliferation and may show lymphocytic infiltrates among sclerotic collagen bundles.
Correct identification and complete surgical resection can prevent recurrence of this rare dermatologic malignancy.
The researchers declared no competing interests.
Reference:
Zhang M, Wu J, Zhang J, et al. Association of indoor tanning regulations with frequency of indoor tanning among US high school students. JAMA Dermatol. 2025;161(3):245-252. doi:10.1001/jamadermatol.2025.0001.