Abstract: This case report details the use of a cellular bone matrix (CBM) and custom titanium mesh (TM) scaffold for vertical bone augmentation in the posterior mandible of a 78-year-old patient. The patient presented with vertical bone deficiency, necessitating augmentation for dental implant placement. The customized titanium scaffold, designed based on CBCT data, provided a precise fit, minimizing the risks associated with traditional TM. During surgery, CBM was used in conjunction with the custom scaffold to enhance bone regeneration. Postoperative recovery was uneventful, with 6-month CBCT scans showing mature bone formation. Histological analysis confirmed successful osseous regeneration. The case demonstrates the effectiveness of combining CBM and custom TM for complex bone augmentation, offering a predictable and stable foundation for dental implants. Future studies with larger sample sizes and longer follow-up times are needed to validate these findings further.
Dental implant rehabilitation in the atrophic posterior mandible is a challenging clinical situation. An assessment of the patient's medical comorbidities as well as clinical and radiographic examination findings help the clinician develop a restoratively driven dental implant treatment plan to ensure a functional long-term result. Short dental implants have demonstrated acceptable long-term survival rates in this region and can be used as an alternative to augmentation in some instances.1-3
If the area of proposed dental implant rehabilitation is planned for vertical bone augmentation, options include guided bone regeneration, titanium mesh (TM), block grafts, interpositional grafts, and distraction osteogenesis. These techniques each have strengths and weaknesses that should be taken into account along with the amount of planned vertical augmentation.4
Advances in digital technology and 3-dimensional (3D) printing allow customized, defect-specific titanium scaffolds to be designed and printed based on the bony topology acquired from a patient's cone-beam computed tomography (CBCT) scan. These customized titanium scaffolds have shown similar vertical bone augmentation effectiveness as traditional TM. However, they do not have the drawback of requiring trimming and shaping of the mesh, which can lead to irregular, sharp borders making the mesh more prone to tissue dehiscence and infection.5-9 If the titanium scaffold is planned for a bone increase of more than 3 mm, studies suggest that at least 50% particulate autograft should be mixed with either particulate allograft or xenograft to maximize graft augmentation.10-13
Autogenous bone grafts are advantageous in osseous regeneration because they have osteoprogenitor cells, osteoconductivity (bony scaffold), and osteoinductivity (bone morphogenetic protein and other cellular signals capable of inducing bone regeneration). Allograft and xenograft materials lack osteoprogenitor cells. Autogenous bone is considered the gold standard but has several disadvantages, including increased surgical time, limited bone volume depending on the harvest site, potential complications at the harvest site, and the need for manipulation into either particulate or contouring to provide a congruent fit into the defect site.
Cellular bone allografts have been used for augmentation of mandibular continuity defects, maxillary implant site development, maxillary sinus augmentation, and periodontal regeneration.14-18 They are typically composed of osteoprogenitor cells, cortical and/or cancellous bone chips, and demineralized bone fibers. Studies have shown them to retain osteoconductivity, osteoinductivity, and osteogenicity.19,20 To preserve the osteoprogenitor cells, these products undergo cryopreservation and require thawing prior to implantation.
The following case report details the use of a cellular bone matrix (CBM) and custom TM scaffold for vertical bone augmentation in a posterior mandible.
Case Report
A healthy 78-year-old male patient presented for consultation regarding fixed prosthetic options for the maxillary left and mandibular right quadrants. Clinical examination revealed a decayed maxillary left canine and a second molar with multiple restorations. In the mandibular right posterior region, missing teeth were noted from the first premolar distal, and an area of black/brown pigmentation was present in the distobuccal tissue of the first premolar, clinically diagnosed as an amalgam tattoo.
A panoramic radiograph generated from the CBCT scan showed a sloped vertical bone deficiency in the right posterior mandible, with limited bone height for dental implant placement superior to the inferior alveolar nerve (Figure 1). The maxillary left quadrant CBCT revealed a decayed left canine with sufficient bone for dental implant placements in the left canine and second premolar locations.
Development of Treatment Plan
A treatment plan was developed for both quadrants. For the maxillary left quadrant, the canine would be extracted with simultaneous dental implant placement, along with an additional implant placed in the edentulous second premolar site. The anticipated final restoration was a three-unit fixed partial denture (FPD).
For the mandibular right quadrant, a decision was made to vertically augment the posterior mandible prior to dental implant placement. Once augmentation matured, dental implants would be placed in the second premolar and first molar areas, with the final anticipated restorations planned as single-unit FPDs. The treatment plans, including alternative options, expected postoperative recoveries, and potential risks, were reviewed in detail with the patient. The patient acknowledged understanding and consented to the proposed treatment plan.
The patient's CBCT was uploaded to the custom titanium scaffold design and manufacturer website portal (Yxoss CBR®, ReOss GmbH, reoss.eu). A mesh design was created, evaluated, and approved (Figure 2). The custom titanium scaffold was then manufactured and delivered. Dynamic navigation implant planning software (X-Guide®, X-Nav Technologies LLC, x-navtech.com) was used to plan dental implant placements in the maxillary left canine and premolar areas.
Initial Surgery
At the time of surgery, the maxillary left canine was atraumatically extracted, and dental implants were placed in the planned positions utilizing the dynamic navigation system (X-Guide). In the edentulous mandibular right quadrant area, a crestal incision with a distolingual release was performed extending mesially in a sulcular manner to the canine region. Full-thickness buccal and lingual flaps were raised, and the periosteum was scored to ensure adequate access and flap mobility for tension-free closure. A cellular bone matrix (Vivagen®, LifeNet Health, lifenethealth.org) was thawed and prepared per the manufacturer's instructions (Figure 3). The titanium scaffold was confirmed to fit acceptably in the defect area, then packed with the CBM and rigidly fixated with 1.7-mm screws (Figure 4). A collagen membrane (Bio-Gide®, Geistlich Pharma North America, geistlich.com) was placed over the scaffold, and the incision was closed with a combination of horizontal and running chromic gut sutures.
Mandibular Implant Placement
The patient had an uneventful postoperative course. A CBCT acquired at 6 months revealed mature bone formation under the mesh at the planned dental implant sites (Figure 5 through Figure 7).
Dental implants were planned and executed with the dynamic navigation software and system (X-Guide) for the mandibular right second premolar and first molar sites. At the time of implant osteotomies, a 2-mm trephine bur was dynamically navigated to create the initial osteotomy for the first molar implant. The bone core from the trephine was sent for histological evaluation (Figure 8). The augmented bone appeared well-healed clinically, and dental implants were placed without complications (Figure 9).
Hematoxylin and eosin (H&E) staining of the biopsy showed a mature graft with signs of new bone formation (Figure 10). An 18-month post-implant placement panoramic radiograph showed acceptable healing in the posterior mandibular right area (Figure 11).
Discussion
This case exemplifies two recent advances in dental implant-specific bone regeneration techniques: the use of a custom titanium mesh scaffold as a space maintainer and CBM as the regenerative material. The utilization of a custom titanium mesh scaffold allowed for a precise fit to the patient's bony defect, enhancing the predictability of the augmentation procedure. Traditional titanium meshes often require significant intraoperative manipulation, which can lead to irregular borders and an increased risk of soft-tissue dehiscence and subsequent infection. Custom scaffolds mitigate these risks by providing a predesigned fit based on the patient's specific anatomy, as acquired from a CBCT scan.
The CBM used in this case provides a unique advantage in bone regeneration. Comprising osteoprogenitor cells, cortical bone chips, and demineralized bone fibers, the CBM retains the essential properties of osteoconductivity, osteoinductivity, and osteogenicity. The cryopreservation process preserves these properties, which may make CBM a viable alternative to traditional autogenous bone grafts in cases such as the one reported here.
The surgical protocol employed in this case involved vertical augmentation with delayed implant placement in the mandibular right quadrant. The choice of a custom titanium mesh scaffold packed with CBM provided a stable and osteoconductive environment conducive to new bone formation. The 6-month postoperative CBCT showed the grafted area had similar radiographic features to the underlying native bone, allowing for the successful placement of dental implants.
Histological evaluation of the bone core obtained during the implant osteotomy confirmed the presence of mature bone, indicative of successful osseous regeneration. This histological evidence, combined with the clinical and radiographic findings, underscores the efficacy of using a custom titanium mesh scaffold and CBM for vertical bone augmentation.
Conclusion
This case report demonstrates the successful application of a custom titanium mesh scaffold and cellular bone matrix for vertical bone augmentation in the posterior mandible. The combined use of these advanced materials facilitated significant bone regeneration, providing a stable foundation for subsequent dental implant placement. The custom scaffold's precise fit, along with the regenerative properties of the CBM, contributed to the overall success of the treatment, highlighting the potential of these technologies in addressing complex clinical situations in dental implantology. Future studies with larger sample sizes and longer follow-up periods are warranted to further validate these findings and refine the protocols for their use.
About the Author
Michael J. Hartman, DMD, MD
Dean's Faculty, Department of Oral and Maxillofacial Surgery, University of Maryland School of Dentistry, Baltimore, Maryland; Private Practice in Oral and Maxillofacial Surgery, Mechanicsburg, Pennsylvania
Figures and Images
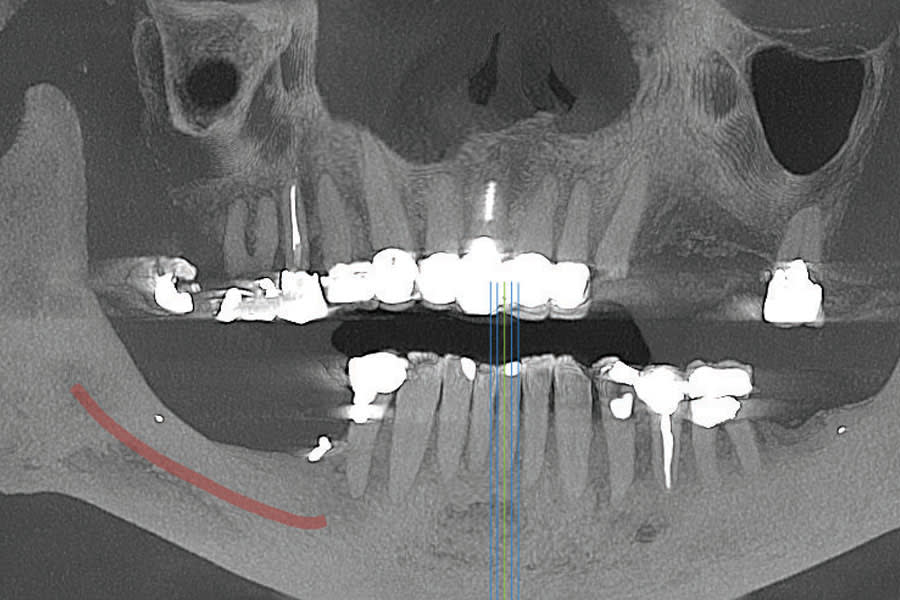
Figure 1
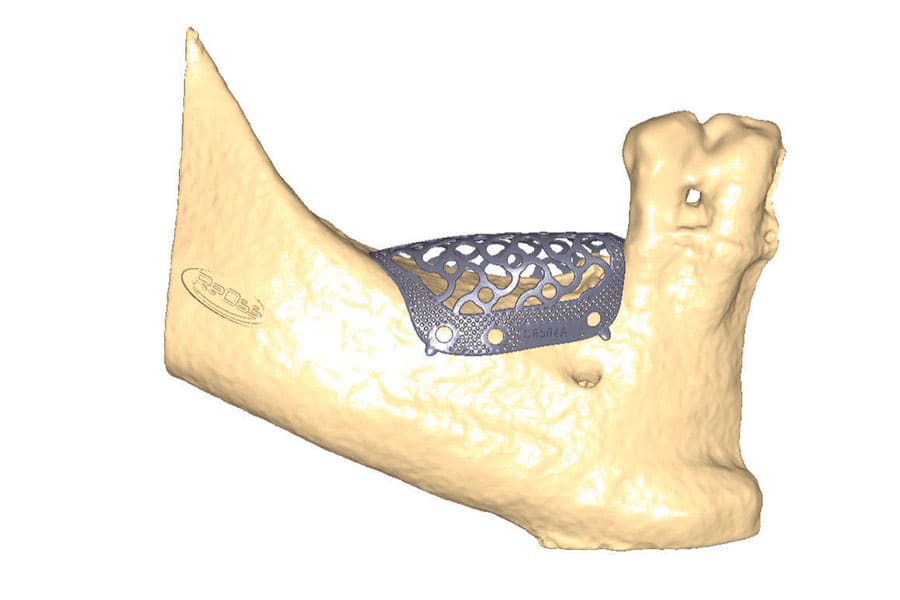
Figure 2

Figure 3
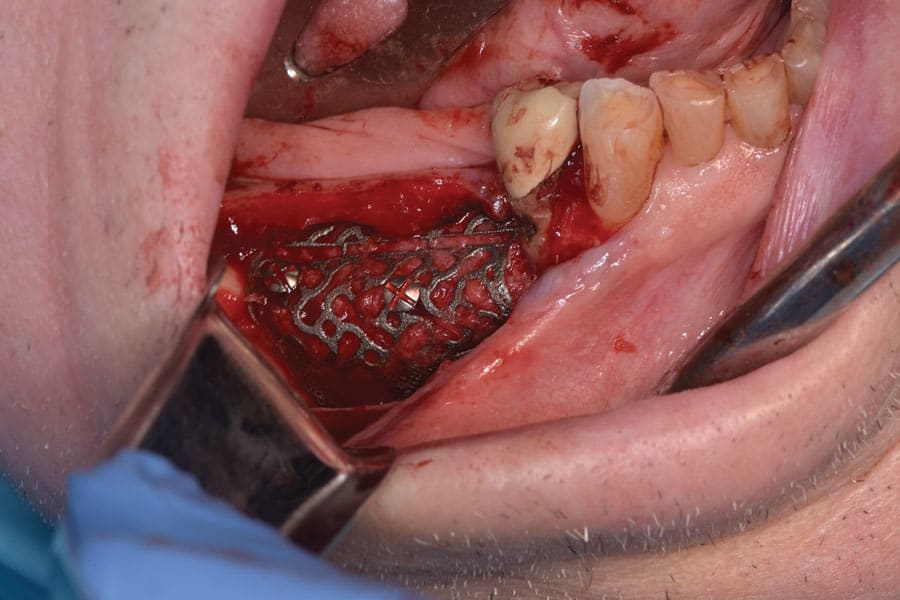
Figure 4
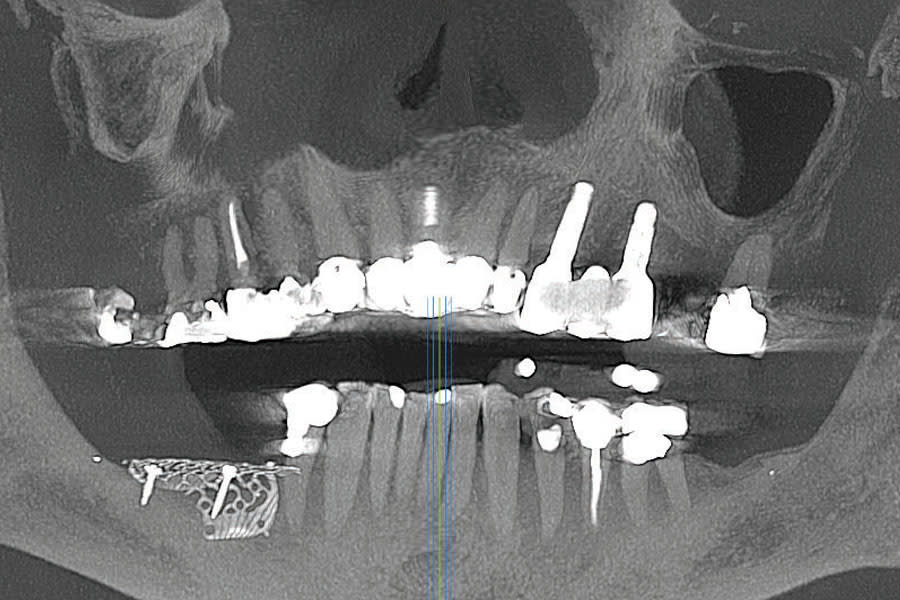
Figure 5
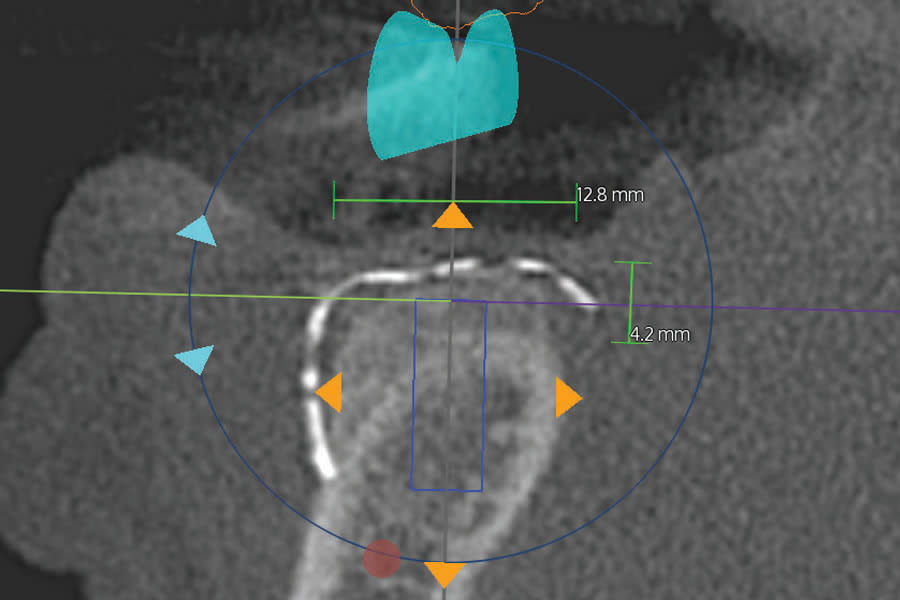
Figure 6

Figure 7

Figure 8
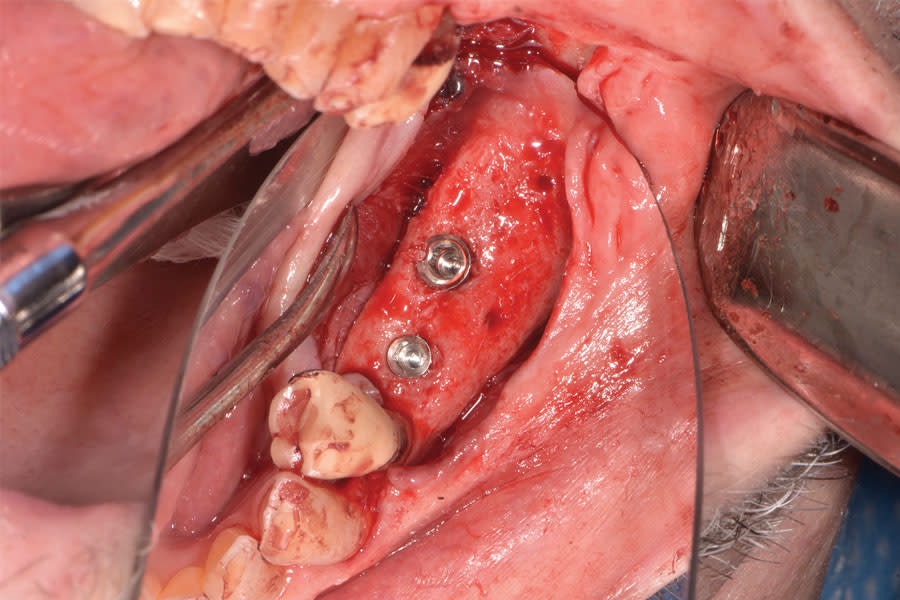
Figure 9
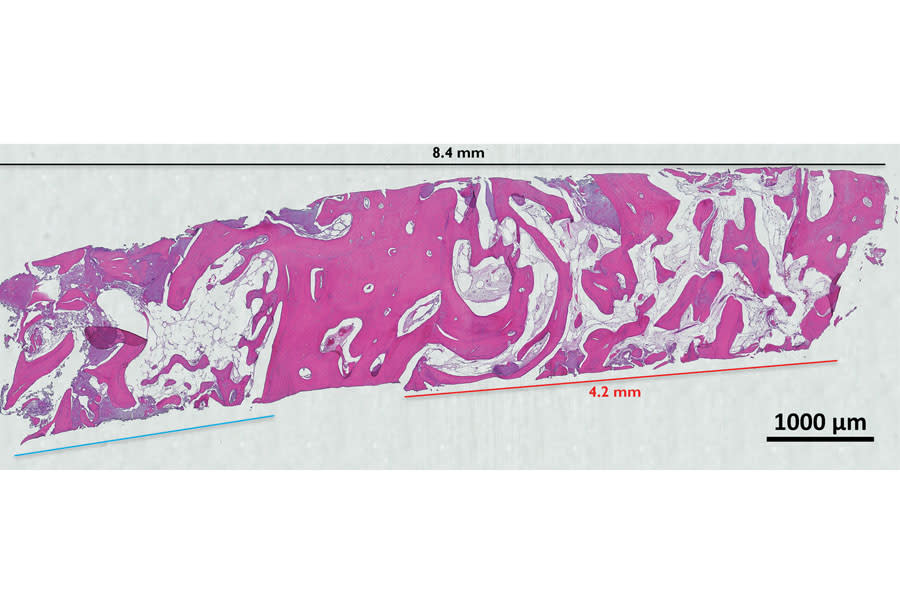
Figure 10

Figure 11